A Single-Site Analysis of the Clinical Profile of Children with Down Syndrome Requiring Enteral Feeding
Thomas Aviles, MD; Danielle Evelyn, MD; Abby Giangiordano, MS, RD; Chunyan Liu, MS; Line Fei, PhD; Ajay Kaul, MD
We aim to describe clinical characteristics of patients with Down Syndrome which are associated with a prolonged need for enteral feeding. We also aim to investigate if any of these factors are associated with BMI outcomes for those who require enteral feeding.
Thomas Aviles, MD & Danielle Evelyn, MD
Abstract
Background: Down syndrome (DS) is a genetic condition involving complete or partial triplication of chromosome 21. Children with DS are disproportionately affected by feeding problems and sequelae of gastrointestinal congenital anomalies. Despite the high proportion of these patients requiring enteral access, there is limited data to guide physicians in managing their enteral nutrition.
Objective: We aim to describe the relationship between age at initiation and duration of enteral feeds, and anthropometrics before, during and at discontinuation of enteral feeds in DS patients.
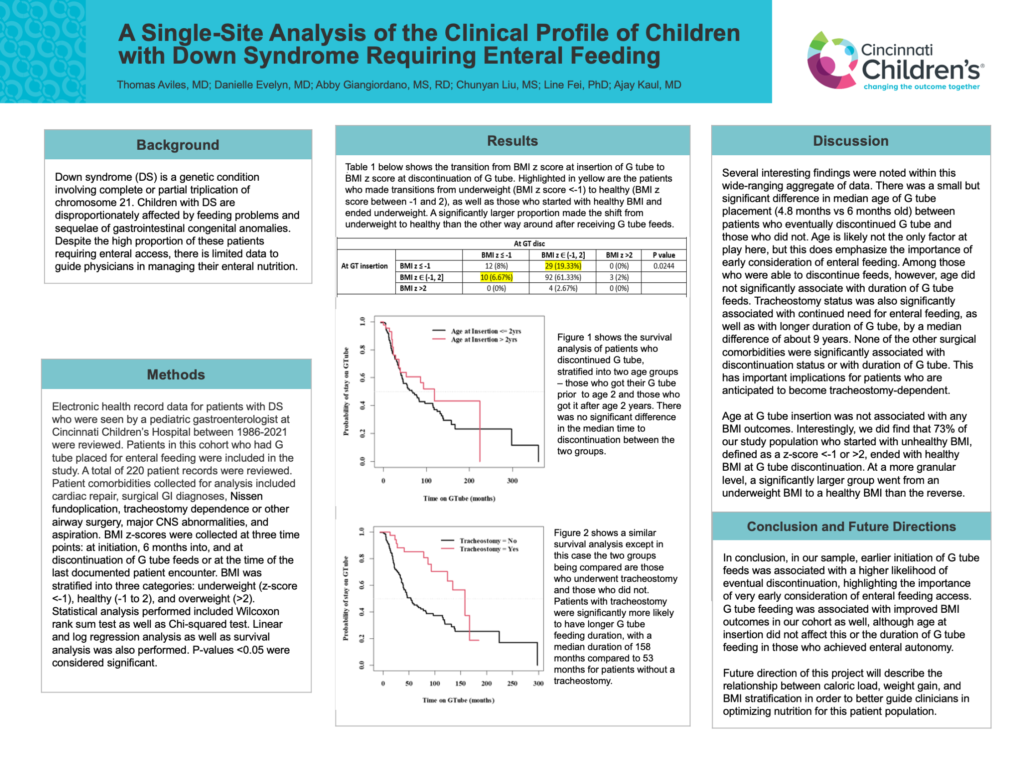
Methods: Children, adolescents and young adults with DS who received enteral feeds and were seen by a pediatric gastroenterologist at CCHMC between September 1986 and December 2021 were included in this retrospective cohort study. Patient characteristics analyzed included cardiac, respiratory, neurologic and gastrointestinal surgical comorbidities. BMI z-scores at G tube placement, 6 months after G tube placement, and G tube discontinuation or last visit were analyzed using regression analysis. Time to G tube discontinuation was also evaluated by Kaplan-Meier estimates and a log-rank test.
Results: A total of 220 patient records were analyzed. Two surgical comorbidities were found to be significantly associated with lower likelihood of discontinuing enteral feeding: brain surgery (2.1% vs 9%, p=0.03) and tracheostomy (12.4% vs 24.6%, p=0.02). Age at G tube placement was significantly younger in those who discontinued G tube versus those who did not (median age 4 months, versus 6 months, p=0.008). There was a trend towards a positive association between earlier G tube insertion (age <2 years at insertion) and shorter duration of enteral feeds. Tracheostomy was significantly associated with longer G tube duration (median duration 166 months vs 66 months, p=0.003). BMI z scores at 6 months after insertion and at discontinuation were not associated with age at G tube placement.
Conclusions: Earlier G tube insertion for DS patients appears to be associated with a higher likelihood of earlier discontinuation of enteral feeds. Those with tracheostomy and/or brain surgery are less likely to discontinue enteral feeding and should be considered for earlier enteral access.